
– How to Fix Insomnia –
5: Consolidation Then Expansion
Whew – I’m relieved you’re visiting this final page, instead of just stopping with the rules on the previous page and getting the impression that I want you to be on a strict and mean sleep schedule and be sleep deprived for the rest of your life. It’s not supposed to be easy, by any means, but neither is it supposed to be a form of punishment. In fact, if done correctly, and you’re able to apply the right amount of pressure on your sleep systems to: 1) get your sleep drive consistently high, 2) your biological clock properly aligned, and 3) your behavioral conditioning pointed in the right direction, you should be able to move on to the next phase within a few weeks or even sooner. You see, there are two main phases of the sleep training period, and the previous page described how to start with the first phase, the sleep consolidation phase.
Phase One: Sleep Consolidation
Why did we just come up with a new sleep schedule? Why is it so important to follow this sleep schedule consistently? The answer: sleep consolidation.
Let’s graph it out. If you’re having trouble falling asleep and staying asleep, a typical night of poor sleep might go like this: You get into bed, toss and turn for a long time before finally falling asleep. Then, you wake up multiple times throughout the night, sleeping in broken chunks. Then, you wake up an hour before your alarm is set to go off, and are unable to fall back asleep so you just lie in bed until it’s time to get up. A graph of this poor night of sleep might look like this:
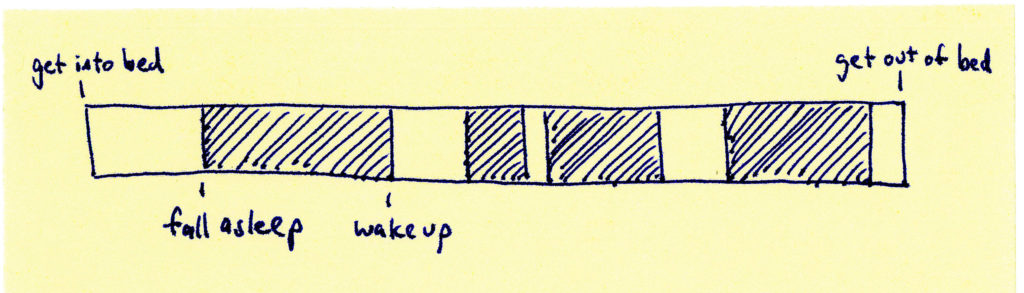
Notice all that time spent in bed not actually asleep. All of that is time spent reinforcing wakefulness in bed. And, if you add up all of the “fragments” of broken sleep and compare it to the amount of time actually spent in bed, it might look like this:
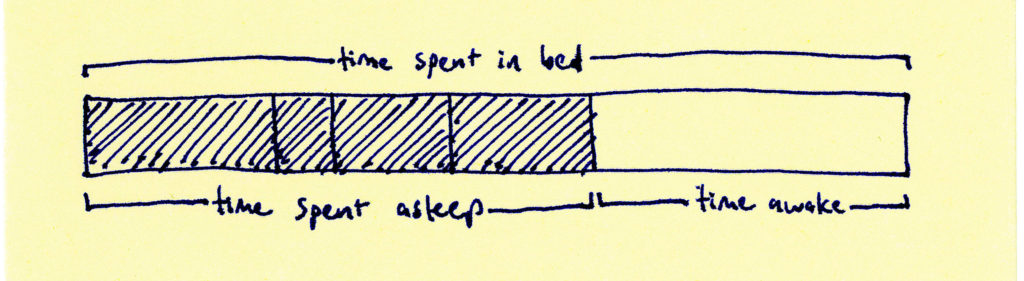
This discrepancy between the amount of time spent in bed and the amount of time spent actually asleep is what we’re really after during the sleep consolidation phase.1 In the steps you took to come up with your new sleep schedule, you calculated this very thing, the amount of time you’re actually asleep on average, and limited your time in bed to roughly around this amount of time. The expected result: your fragmented sleep will turn into consolidated sleep. The sleep you experience in broken segments should fuse together and cause you to fall asleep much faster and stay asleep better.
Think about all that time you’re in bed but not asleep, whether trying to fall asleep, waking up in the middle of the night, or waking up too early before your alarm. Remember, this time is spent reinforcing wakefulness in bed, which makes it more likely for this to happen in bed the next time and the next time. That’s why we need to cut out all of the time you’re not in bed. So logically, if you’re only getting, say, 5.5 hours of sleep per night, and trying to cut out all awake-time in bed, you should be spending in the ballpark of 5.5 hours in bed. Another way I explain to clients is: if it takes you an hour on average to fall asleep after getting into bed, then you should be spending that hour outside of bed so as to increase the sleep drive and engage in behavioral conditioning – thus a one hour later bedtime would be a good start.
How do I know if it’s working?
You should start to experience your body responding to your new sleep schedule and behavioral changes over the first week. Like I mentioned before, one of the first things you will notice is feeling more sleepy during the day and close to bedtime. This should happen within the first 4-7 days. In fact, I advise that you prepare for this by planning activities that will help you stay up until your bedtime, instead of falling asleep on the couch watching TV (extremely common mistake). Then, over the course of the next days to weeks, you will start to notice being able to fall asleep quicker, waking up less often and long, and having more consistency (i.e. less irregularity) in your sleep drive in the evenings.
The sleep consolidation phase typically lasts 1-3 weeks before the participant is ready to move onto the next phase, sleep expansion. Regularly assess your sleep using the bullet points below to determine if you’re ready to move on. Note: if you don’t feel any of those effects mentioned above (increased sleepiness, falling asleep quicker, staying asleep better), you may need to shorten the duration of “time in bed” by making your bedtime later. However, as mentioned before, I don’t recommend restricting your time in bed to less than 5.5 hours.
Whereas phase one is about first increasing the quality of your sleep (through consolidation), phase two is about increasing the quantity of your sleep.
Phase Two: Sleep Expansion
- Feeling sleepy by the time you reach your new bedtime?
- Falling asleep within 30 minutes of getting into bed?
- Awake for less than 30 minutes total in the middle of the night?
If you’ve answered yes to all three of these questions, this indicates that you’re ready to move onto the sleep expansion phase. It means that your body is responding to the new sleep schedule and the behavioral changes as we hoped, and that your sleep is becoming consolidated.
As I promised before, the sleep schedule you came up with for the first phase is not a permanent schedule – it is just a means to an end: consolidated sleep. These schedule changes and behavioral changes are just part of a training period that is temporary, to help you go from being stuck in a pattern of poor sleep to actually “being stuck” in a pattern of good sleep.
Sleep expansion steps
- Assess if you’re getting sleepy by bedtime, falling asleep quickly, and staying asleep adequately (bullet points above).
- If yes, add 15 minutes to your sleep schedule by moving bedtime earlier.
- If no, continue with current schedule. (If you’re repeatedly unable to get to yes, try moving your bedtime even later. If this doesn’t work, consider assessing for other causes of the poor sleep and/or seek professional help.)
- Stick with this new schedule for about a week (at least 4 days) before re-assessing and adding more sleep time – back to step 1.
- Eventually you’re going to reach a point where your body will tell you to stop the sleep expansion. You will no longer consistently be able to answer yes to all 3 questions. Stop there – this is the sleep schedule you should adopt and maintain for the time being. If you want to keep adding more sleep, wait a few weeks and re-assess.
This is a pretty simple and effective way to do the sleep expansion phase. It isn’t an exact science or math, so feel free to adjust as you see fit and not get so hung up on the exact numbers. If you’re more data driven, you may want to calculate sleep efficiency using sleep logs or measure your sleep using sleep trackers. In that case, try to get to 90% for your sleep efficiency score2 before adding the 15 minutes to the sleep schedule. Even this method is subject to flaws in self-reporting (sleep logs) or technological/algorithmic limitations (sleep trackers) so take the data with a grain of salt when you make decisions about adjusting your sleep schedule.
As you can see, the point of the sleep expansion phase is to very slowly increase the amount of sleep you get per night until your body reaches an equilibrium point. Larger increments than 15 minutes may certainly be fine, but being on the safe side with the smaller increments and 4-7 day trial periods increases the likelihood you’ll be able to hold onto the sleep efficiency gains you’ve made while expanding your sleep schedule.
Wait, when do we talk about sleep hygiene?
Glad you asked, and… right now! Once you’ve reached the sleep expansion phase, that is when I believe good sleep hygiene becomes more important. Sleep hygiene is a funny word, if you’ve never heard of it before, which just means sleep related behaviors and routines. Most practitioners delivering CBT-I will put the sleep hygiene education and implementation first (and I used to do this too) but I have found that overall the intervention is most effective when you focus first on the “biggest bang for your buck”, which is targeting the three systems and consolidating your sleep. Plus, even if your sleep hygiene may be less than stellar, your body should still respond to the sleep consolidation phase, resulting in increased sleep drive, faster sleep onset, less awakenings, and a more consistent circadian rhythm. Thus, it is when you reach the sleep expansion phase and you start to decrease the pressure on the sleep drive that you’ll need to make sure you’re paying attention to maintaining helpful sleep-related behaviors and practices, and optimizing the other variables in order to help you maintain the gains.
- Create a comfortable sleep environment – including mattress comfort, temperature, minimizing noise and light exposure, etc.
- Unplug from your electronic devices (especially the ones that emit sleep-disrupting blue light) at least 30-60 minutes before bed and don’t take them into bed with you.
- Exercise regularly, but not too close to bedtime (within 3 hours before bedtime).
- Establish a consistent wind-down routine 30-60 minutes before bed that focuses on getting physically and mentally relaxed. Learn and practice ways to reduce anxiety.
- Reduce the use of alcohol, caffeine, and nicotine, especially close to bedtime. General rule of thumb: avoid alcohol after dinner, caffeine after mid-afternoon, and nicotine 2-3 hours before bed.
Final thoughts
Congratulations, you’ve made it to the end of my guide. I really hope that you have found this helpful, and that you will be able to put into practice some of the things you’ve learned in order to improve your sleep. Behavior change is not easy, and that’s why it takes a period of training and discipline in order to change your sleep patterns for the long term. It isn’t as if the mere act of learning this information can automatically fix your sleep problems. But if you think about the many months and likely many years of poor sleep you have been dealing with, and compare that with 4-8 weeks of sleep training you’ll need to undergo in order to drastically improve your sleep and get “stuck” in a pattern of good sleep, my guess is that you’ll find this prospect worthwhile.
I have tried to keep this guide focused on the most important elements of a behaviorally-based insomnia intervention and wasn’t able to include other optional or advanced topics. Feel free to browse the site to learn more. Thanks for visiting!
- In CBT-I, this is an important calculation and has a name, the sleep efficiency score. Simply, this is a ratio of hours asleep / hours in bed. The target sleep efficiency is 90% (meaning that you’re aiming to be asleep 90% of the time you’re in bed), while people with insomnia typically start in the range of 60% – 80%.
- Your sleep efficiency score = number of hours asleep / number of hours in bed. Calculate your sleep efficiency weekly (or rolling 7-day average) to assess if you should add more time to your sleep schedule. If you are getting sleep efficiency scores in the 75% or below range during the sleep restriction phase, try decreasing your time in bed by going to bed 15 minutes later. Reminder: I don’t recommend scheduling less than 5.5 hours for bed.